Reviewing Coding in the Detailed Visit Overview (iPad)
Encompass supports the latest Evaluation and Management (E/M) coding requirements. Encompass simplifies the coding process by suggest billing codes supported by your clinical documentation and based on AMA and CMS requirements. By default, Encompass autocodes exams based on medical decision making (MDM); however, you have the ability to review the coding at every step of the way, and you have the option to override the complexity level of the case or override the suggested billing code. You also have the ability to code the visit based on the time spent by clinical staff rather than basing the coding on MDM.
Encompass streamlines the coding process while giving you the ability to exercise your professional judgment. Watch the following videos for an overview of E/M coding in Encompass and read the topics below for more detailed instructions.
What do you want to do?
Medical decision making is based on three criteria:
- Number and complexity of diagnoses or treatments
- Amount or complexity of data to be reviewed
- Risk complications, morbidity, or mortality
You must document at least two of these criteria.
To streamline your workflow, Encompass automatically calculates MDM based on your exam selections. To this end, thorough exam documentation is essential to ensuring you're billing at the highest appropriate level.
- Document and verify the complexity of all diagnoses and associate diagnoses. Diagnoses contribute to the complexity. Each diagnosis and associated diagnosis in Encompass has been assigned a default complexity based on AMA guidelines. For more information, go to Understanding the Default E/M Complexity in Encompass.
- Document all tests performed. Tests contribute to the data reviewed. Tests have been assigned a default complexity.
- Document all medications prescribed and decisions associated with plans. Medications and decisions contribute to the risk of complication. Plans and medications have been assigned a default risk complication, morbidity, and mortality level.
- Open a patient visit. To learn how, go to Creating or Opening a Visit (iPad).
- Tap Documents.
The Visit Note screen appears with the preliminary visit note displayed.
- Tap the Encounter tab
along the left side of the screen.
The Encounter Form displays a breakdown of the current exam's calculations, including the level of MDM and the number/complexity of problems addressed.
You can adjust the complexity of diagnoses and associated diagnoses to ensure that Encompass calculates the estimated E/M code for the visit is accurately.
- Open a patient visit. To learn how, go to Creating or Opening a Visit (iPad).
- Swipe up to the Impressions and Plans section.
- Locate the diagnosis and tap the Complexity and Status link.
The Select Complexity and/or Status window opens.
- Tap the Presenting Problem Complexity drop-down menu and select a complexity.
Every diagnosis is assigned a default complexity based on AMA guidelines. Tap the Definitions link to learn more about the complexities.
- Select a Status as needed.
Selecting a Status is optional and does not impact billing.
- Tap Done.
- Open a patient visit. To learn how, go to Creating or Opening a Visit (iPad).
- Swipe up to the Impressions and Plans section.
- Locate the associate diagnosis and tap Edit.
The Associated/Cause Dx screen opens.
- Tap the Complexity and Status link.
The Associated Dx Complexity window opens.
- Select a Complexity and tap Save.
Every diagnosis is assigned a default complexity based on AMA guidelines. Tap the Definitions link to learn more about the complexities.
- Tap Done.
- Open a patient visit. To learn how, go to Creating or Opening a Visit (iPad).
- Locate the CC/HPI|ROS section header, tap the Add CC/HPI or ROS drop-down, and select Independent Historian.
The Add Independent Historian screen opens.
- Tap the Who Provided this History for the Patient? drop-down menu and select the appropriate person.
- Tap the Why was this History Provided by an Independent Historian? and select a reason.
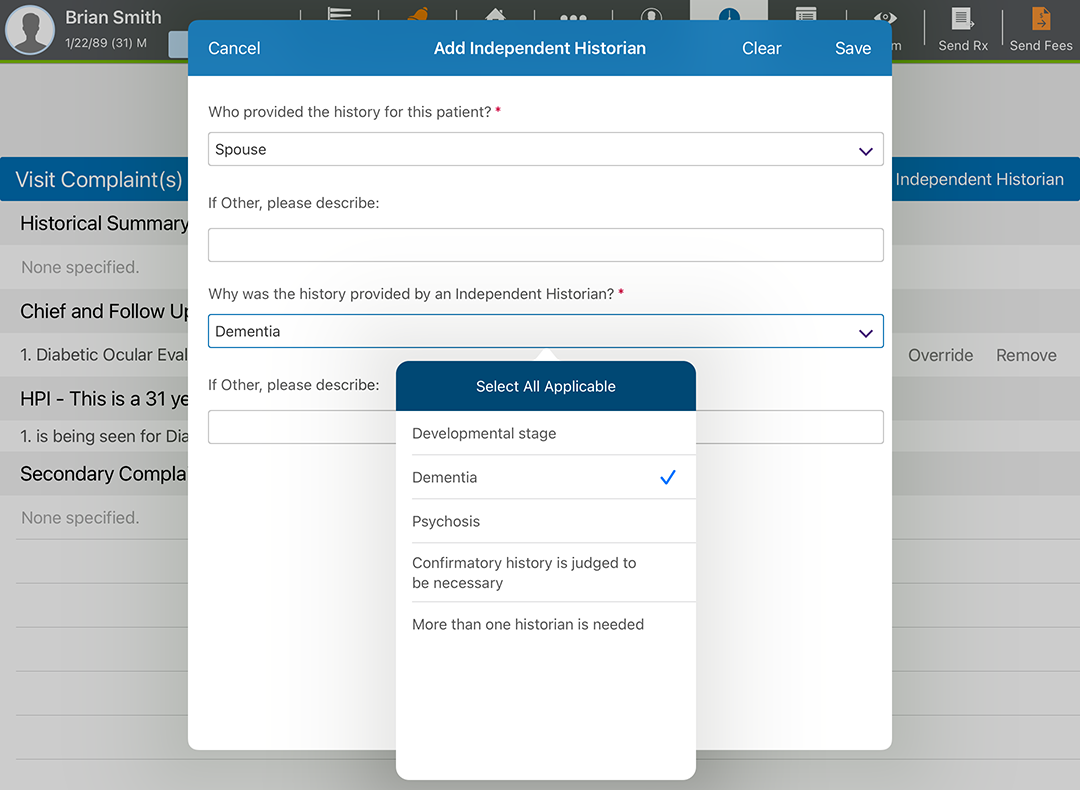
- Tap Save.
As an alternative to billing based on medical decision making, the code level can be based on physician time for face-to-face, in-office services. Time may include preparing to see the patient; ordering medications, tests, or procedures; and care coordinations, as long as these activities occur on the same day as the visit.
- Open a patient visit. To learn how, go to Creating or Opening a Visit (iPad).
- Swipe up to locate the Billing section.
- Tap Override Billing and select Bill Visit Based on Time.
- Enter the Total Time (minutes).
- Tap the Time Spent on the Following drop-down menu and select one or more activities.
- Tap Bill by Time when you’re finished.