Support Electronic Referral Loops by Receiving and Reconciling Health Information
The objective of this measure is to conduct a clinical information reconciliation for medications, medication allergies, and current problems for at least one patient—who was referred to you as a transition of care or for a patient whom you have never before encountered—and for whom you have received an electronic summary of care record during your performance period.
See also Publishing Your Digital Contact Information
This objective of this measure is to encourage you to incorporate patient health information sent by other clinicians into the patient’s record. You should, whenever possible, request that the summary of care (CCD) be sent electronically via direct mail.
This process requires two actions:
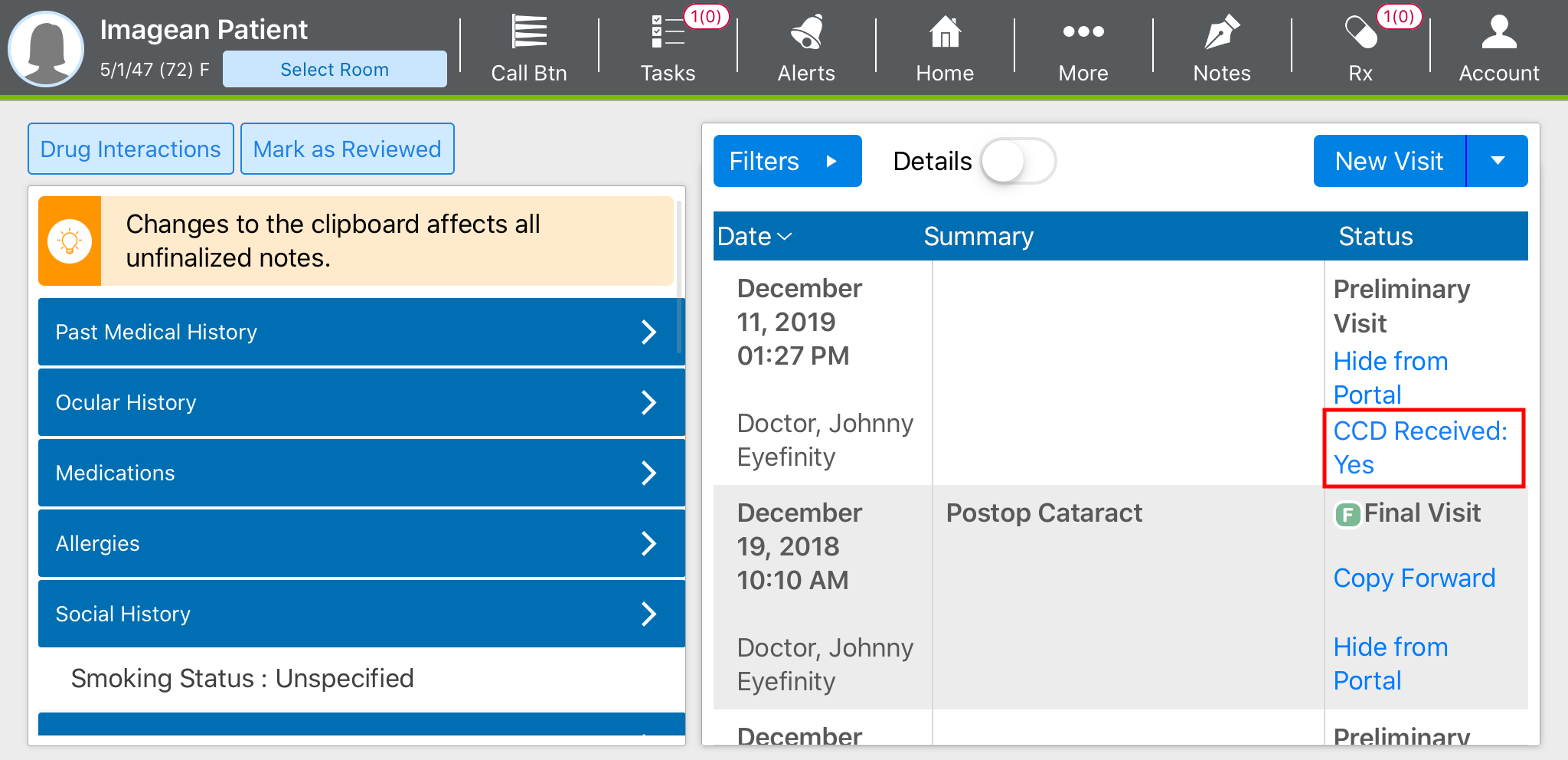
If you do not receive a CCD from the referring provider, tap CCD Received: Yes under the exam status so that it changes to "CCD Received: No." If you don't set the CCD Received indicator to "no," the exam will count against your performance in this measure.
Receiving Summaries of Care
To complete this task, you will need a secure message with a summary of care (CCD) attached, and a preliminary visit with which to associate the CCD. When you receive a secure message containing a CCD file, perform the following steps:
- In Encompass, tap Mail.
- Select the Direct Mail Inbox.
- Tap the subject of the message.
- In the Attachments section, locate the CCD and tap Associate with Patient.
- The Document Management page opens.
- Enter the name of the Patient, select the Visit, and ensure the Category displays CCD.
- Tap Save.
Incorporating Summaries of Care into Patient Records
Once you’ve associated the summary of care with an exam, you’ll need to incorporate the medication, medication allergy, and problem list data into the patient’s record:
- Open the preliminary visit.
- Open the patient clipboard:
- Tap More.
- Select Patient Clipboard.
- Tap Edit.
- Reconcile any medications:
- Tap the Medications tab.
- Tap Import.
- Select Transition of Care (CCD).
- Review the medications.
- Tap Select All or tap to select individual medications manually, as needed, and tap Accept.
OR
Tap Reject to not incorporate any of the medications into the patient’s record.
A summary page lists the patient’s current medications and highlights the medications that will be imported from the CCD.
- Tap Accept.
- Tap Back to exit medications and return to the patient clipboard.
- Reconcile any medication allergies:
- Tap the Allergies tab.
- Tap Reconcile.
- Select Transitions.
- Review the allergies.
The left side of the screen displays the allergies currently in the patient record. The right side of the screen lists the allergies included in the CCD, including the date recorded, the author, reaction, and severity. You may need to swipe up to see additional allergies.
- Tap Select All or tap to select individual allergies manually, as needed, and tap Accept.
OR
Tap Reject to not incorporate any of the allergies into the patient’s record.
A summary page lists the patient’s current allergies and highlights the allergies that will be imported from the CCD.
- Tap Accept.
- Tap Back to exit allergies and return to the patient clipboard.
- Reconcile the problem list:
- Tap the Problem List tab.
- Tap Reconcile.
- Select Transitions.
- Review the problems.
The left side of the screen displays the problems currently in the patient record. The right side of the screen lists the problems included in the CCD, including the date recorded and author. You may need to swipe up to see additional problems.
- Tap Select All or tap to select individual problems manually, as needed, and tap Accept.
OR
Tap Reject to not incorporate any of the problems into the patient’s record.
A summary page lists the patient’s current problems and highlights the problems that will be imported from the CCD.
- Tap Accept.
- Tap Done to exit medications and the patient clipboard.
The reconciliation is now complete. Continue documenting the exam.
This objective of this measure is to encourage you to incorporate patient health information sent by other clinicians into the patient’s record. You should, whenever possible, request that the summary of care (CDA) be sent electronically via secure messaging.
Importing and Reconciling the Summary of Care
Prior to the patient's appointed visit, import the transition of care file:
- In the Control Center, search for the patient.
- Click Patient Hx.
- Click the eDocuments tab.
- Click Import CDA – Transition of Care.
- Locate the CDA file, select it, and click Open.
The CDA Reconciliation window opens.
- For each element that you’d like to import into the patient’s record, select the Import check box. At a minimum, you must reconcile the medication, medication allergy, and current problem list.
- Click Save.
Documenting the Exam
To receive credit for this measure, you must code the exam as a referral or transition of care and review the medication, medication allergy and problem lists:
- In the Control Center, search for the patient and create a new exam.
- Select referral as the reason for visit:
- Click the Reason for Visit category bar.
- Select one of the Referred By radio buttons.
- Review the medications and medication allergies:
- Click the Patient History category bar.
- Select the Medications - Systemic/Ocular/Allergies check box and click Process.
- Edit or add notes to the medications and medication allergies listed.
- Click Medication Reconciliation.
- Click Medication Allergy Reconciled.
- When finished click Save/Exit.
- Review the problem list:
- Click the Patient Hx toolbar button.
The Patient Information Center window opens.
- On the Exam Hx tab, click Maintain Problem List to make any changes.
- Click Problem List Reconciled.
- Click the Patient Hx toolbar button.
- Link the CDA to the exam:
- With the Patient Information Center window still open, click the eDocuments tab. If this window is not open click the Patient Hx toolbar button.
- In the Patient Electronic Documents list, locate and double-click the recent CDA Import - Transition of Care document.
- Select the Attach Document to Exam check box.
- Click Save/Exit.
The Exam No. and Link check box should now be populated for the CDA Import - Transition of Care document.
- Click Exit when you are finished.
- Code the exam as a new patient or transitioned patient exam:
- Click the Coding toolbar button.
- Click the Procedures tab.
- Select an exam for a new patient or transitioned patient (92xxx or 992xx).
- Complete the rest of your coding and Save/Exit.
- Document the remainder of the exam and Finalize.
For at least one electronic summary of care record received for patient encounters during the performance period for which a MIPS-eligible clinician was the receiving party of a transition of care or referral, or for patient encounters during the performance period in which the MIPS-eligible clinician has never before encountered the patient, the MIPS-eligible clinician conducts clinical information reconciliation for medication, medication allergy, and current problem list.
Denominator
Number of electronic summary of care records received using a certified EHR for patient encounters during the performance period for which a MIPS-eligible clinician was the receiving party of a transition of care or referral, and for patient encounters during the performance period in which the MIPS-eligible clinician has never before encountered the patient.
Numerator
The number of electronic summary of care records in the denominator for which clinical information reconciliation is completed using a certified EHR for the following three clinical information sets:
- Medication. Review of the patient's medication, including the name, dosage, frequency, and route of each medication.
- Medication allergy. Review of the patient's known medication allergies.
- Current problem list. Review of the patient’s current and active diagnoses.
The numerator must be one or more.
Any MIPS-eligible clinician who receives transitions of care or referrals or has patient encounters in which the MIPS-eligible clinician has never before encountered the patient fewer than 100 times during the performance period.
This measure is required to achieve a promoting interoperability score. This measure is worth 15 points.
The following are suggested roles for completing this measure:
- Doctor
- Technician
- Scribe